One day, software will have eaten healthcare. That day has not come yet, but it will. And it’ll come just in time.
First of all, what do we mean when we say “software eats ___”? What it doesn’t mean is, ‘take existing industry, add software’. Software eats the hotel industry doesn’t look like the Hilton app, it looks like Airbnb. Software eats payroll doesn’t look like the ADP website, it looks like Zenefits. When software eats an industry, the software isn’t actually what matters most; the exciting parts are the new business models that emerge.
So when we talk about software eating healthcare, we’re not actually talking about health apps, telemedicine, or internet doctors. They might be neat, but they mostly miss the point. We’re talking about software accelerating our transition towards new healthcare business models that have lower costs and better outcomes. It hasn’t happened yet in healthcare, because healthcare is hard. But we’ll get there, and this post will try to illustrate with a simplified framework (particularly for those who are outsiders to healthcare) the following:
1. The problem: Why healthcare is so expensive, and why software hasn’t really made a dent yet.
2. The mechanism: How bundling and unbundling drive change in the healthcare industry. jump to section
3. The playbook: How to understand the change that’s happening now, and how it creates the conditions necessary for software to eat healthcare. jump to section
4. Wrapping up with my final thoughts on “Software Eats Healthcare”. jump to section
(One note before we begin: I am not talking about software eating biology or even medicine. Biology and medicine are in the realm of science; health care is a business. They’re both important, but I’m focusing on the latter.)
1. The problem: Fee for service.
Anyone with an ear towards the news has probably heard the debate over how we pay for health care: single payer vs. employers, Obamacare, insurance exchanges, and much more. But for the uninitiated, if you want to understand one thing about health care, make it this: how we pay for healthcare is actually less important than what we pay for when we pay for healthcare. Today, when we purchase health care in most cases we are paying a fee for service: you go to a health care centre, receive care, and the care provider bills the payer (whether it’s your insurance, the government, or out of pocket) on a predetermined fee schedule.1 In essence, you’re paying in a similar manner to how you’d pay a lawyer, a consultant, or some other expert.
This seems normal to us, because we haven’t really experienced any alternatives. But there actually three ways that we could be paying:
-Fee for service (You pay for a treatment, procedure, or simply the doctor’s time: nearly all of the cost is marginal)
-Fee for outcome (You pay for a result, or a successful outcome of a procedure: more of the cost is fixed and upfront, since procedures are relatively standardized)
-Fee for health (You pay for health, i.e. potentially not needing a procedure at all: nearly all of the costs are fixed and up-front)
Before passing judgment as to which of these are ‘better’, consider the fact that each of these business models makes sense in specific circumstances. Fee for service is the correct business model for situations when problems or solutions are unknown, and you need to pay for expertise in order to discover an appropriate remedy. For internal medicine, emergency room care, and other medical situations that can be highly uncertain or ambiguous, fee for service is logical. However, most health care problems aren’t like that. If I have a fractured hip and need a rehabilitation program, or even just a cold and need medicine, your problem (and solution) are known. You should be paying for an outcome – a successful procedure or program – not paying for the service itself. And finally, if I have early stage type 2 pre-diabetes, the goal shouldn’t be to provide me with more health care: the goal is to get me healthy again through behavioural interventions so that I don’t need expensive care later on, period. I shouldn’t be paying for service or for outcome – I should be paying to attain and maintain a state of health.
The big problem with health care today (regardless of who is paying) is that we’re stuck paying for the most expensive parts of health care – chronic illnesses and behaviourally dependent conditions – with a fee for service business model. It’s also why the technical innovation we’ve seen recently – in biotech, genetics, pharmacology, or software – hasn’t really driven down the cost of care for long-term chronic conditions yet. When you’re paying fee for service, new innovation piles up at the high end but doesn’t actually lower costs much; it mostly increases the amount of care that’s possible to administer. This isn’t ideal. And up until now, software hasn’t had a transformative impact the way it has in other industries: when we’re stuck with fee for service, the only way to control costs is to lower the amount of services you perform – and no amount of software, however well designed, can really incentivize anyone to do that. Software can’t eat healthcare yet; we’re not ready.
That, in a nutshell, is the problem. And if nothing changes, we could be in serious trouble: fee for service healthcare plus an aging population could bankrupt everyone and that would be #bad. But things will change: with any luck, software will eat healthcare just in time. And in doing so, it will accelerate our transition towards fee for outcome and fee for health business models that don’t just cost less, they also give better results.
The big question is: how is this going to happen?
2. The mechanism: bundling and unbundling make the world go ’round.
There are a lot of factors that contribute to health care quality, cost and change – far too many to list here. But there is also one simple but powerful force at work in the background, and it’s the same force that drives change in other industries: the bundling and unbundling cycle. Jim Barksdale told us in the leadup to the Netscape IPO, “There are only two ways I know of to make money: bundling and unbundling.” And as I’ve written about previously, this maxim applies just as much to health care as it does to software. Incremental improvements drive incremental change; bundling and unbundling drive the massive, systemic changes that lurch health care forward.
What have they looked like so far? It helps to think about the health care industry in terms of its fundamental units. A century ago, the fundamental unit of health care that mattered was the physician. They provided health care, and they were the billing authority – the health care industry, for all intents and purposes, was a collection of doctors. Then, during the 20th century, we went through a bundling cycle: physicians were bundled into health centers. The big units of health care that mattered became the clinics, the hospitals, and the university networks.2 This bundling cycle made sense: there was a lot of efficiency to be gained through shared resources, staff, equipment, purchasing power, and all of the other benefits that come from a merged business. Health care became a collection of health centers. For a while, this worked out ok.
Then we ran into a problem. The general hospital, for all its efficiency of resources, turned out to be a very inefficient business model when it came to innovation and cost control. The problem has to do with fee-for-service: when a health center runs on a unified business model that makes money for providing service (as opposed to providing results, or providing health), that center is incentivized to provide as much care as possible, and the most expensive care possible. Furthermore, despite advances in research and technology significantly increasing our standards of care, costs increased in alignment with the fee-for-service business model. This is very hard to fix without a significant change in the way things work: an unbundling was required.
The first attempts at unbundling the general hospital and health care centers, unsurprisingly, came at the high end; also unsurprisingly, they didn’t work. Here’s what happened: clinicians and entrepreneurs began thinking critically about the jobs they were doing that were once difficult, but through years of research and improvements had become relatively routine. Certain surgical procedures, for instance, had become standardized and reliable enough that the obvious business model for them should be fee-for-outcome, not fee-for-service. So they founded specialty clinics that could hyper-specialize, guarantee an outcome, and charge competitive prices based on higher fixed + lower marginal costs: an attempt to unbundle the general hospital, starting with the most expensive and lucrative jobs. So what happened? The hospitals said F that! Those surgical procedures were money-makers for the big health centers – they weren’t surrendering them without a fight. And as powerful incumbents usually do, they raised all sorts of hell about safety and regulations, effectively blocking these specialty shops from opening. (There’s a revealing exception: hospitals had no problem whatsoever allowing psychiatric patients, who have never been profitable, to be unbundled to specialty mental health centers. The exception further proved the rule.) Health care stayed stuck with blanket fee-for-service in bundled centers; the incumbents won.
But then, something surprising happened: an unbundling catalyst appeared, in the form of a Trojan Horse. That catalyst was Electronic Health Records. EHRs, which were demanded for years but very hard to deploy, were sold to the hospitals on an incumbent-friendly value proposition: efficiency. And after decades of development and deployment, we finally got to see EHRs get deployed into hospitals and…people hated them. No one liked the new systems, they didn’t obviously show a significant visible improvement over the paper files, and they generated a lot of whining overall. (As far as software goes, for the most part they weren’t great code.) And yet for all of these complaints, EHRs have been an enormous success: they created a mechanism to lower costs across the whole health care stack.
How’d they do this? Because they introduced a way for hospitals and health centers to unbundle all of thelow-end services that were expensive but not profitable. Instead of getting your weekly blood pressure checkups or diabetes treatment at an expensive health center, you can now go to the retail clinic at the local pharmacy. You’ll get that job done for less money, in a fundamentally lower-cost business model: fee for outcome, where more of the costs are fixed (building and staffing the retail clinic) and the marginal cost of an additional checkup is very low. Health centers were okay with this, because they weren’t making money on those blood pressure checkups anyway! They’ll happily let that service get unbundled to cheaper, ‘inferior’ retail clinics. This is classic Innovator’s Dilemma 101: unbundling at the low end is how disruptive business models take hold, especially in heavily regulated complex industries like healthcare. EHRs provided the catalyst for the unbundling of the health center into distinct jobs, starting at the low end and now working its way up towards more complex treatments and procedures. Physicians got bundled into centers, and now centers are slowly but surely being unbundled into new fundamental units: the jobs they perform.
Still with me? We’ve got some more to go- we’re still not at a point where software can eat healthcare. We’re making progress, but we’re still going to need one more turn of the bundling-unbundling cycle before we get there.
The playbook: how one more turn of the bundling cycle will let software finally eat healthcare.
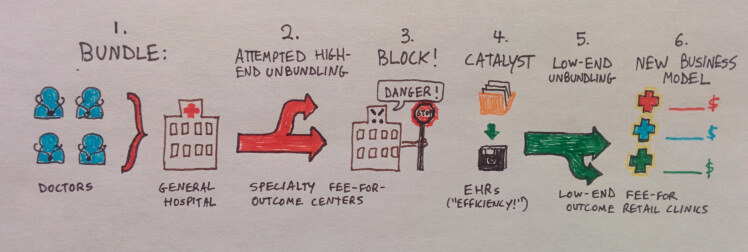
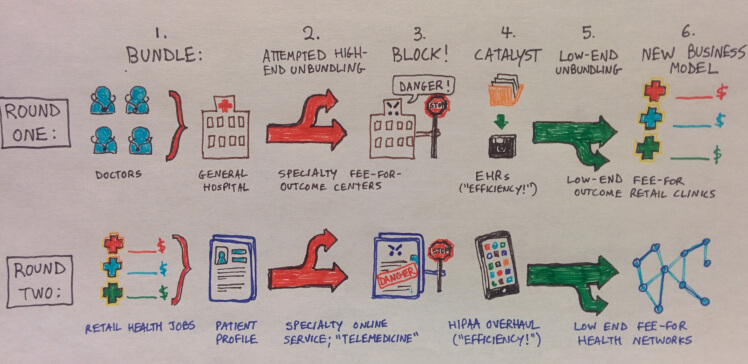
Let’s recap. We’ve seen one full turn of the bundling-unbundling cycle so far: 1. Doctors got bundled into centers; 2. the attempted high-end unbundling of specialty fee-for-outcome clinics; 3. successful block by incumbents protecting their profit centers; 4. an unbundling catalyst appears (EHRs); 5. an unbundling at the low end (retail clinics) into various jobs; and 6. the emergence of new lower-cost business models for each of these jobs.
However, despite this progress, we’re not yet at a point where software can really eat healthcare. Why not? Because the jobs that have emerged as principle components of health care, however efficient that they are, are still being done in isolation from one another. And software doesn’t do well in isolation: an Airbnb network with one person isn’t very helpful; Zenefits with only one company isn’t either. Something important is required before these new network business models can emerge in healthcare: alignment and connectivity between isolated jobs. We need to be able to harness the fact that the millions of people fighting diabetes, depression, back pain, Alzheimer’s, and just about every chronic expensive condition you can think of all have more or less the same goals as their peers. This is where the software and the internet can potentially make a staggering difference. So how are we going to get there?
“All of this has happened before, and all of it will happen again.” -Battlestar Galactica; also applies to software eating health care
If you guessed ‘another bundling and unbundling cycle’, we agree! And my bet is that Round Two of the cycle will look very similar to Round One. The actors will be different, but the motives will be the same. And this time, the outcome will be network conditions where software can fundamentally transform the way we manage chronic issues and preserve healthy states for everyone.
The first phase of the cycle (which is already happening) is the component jobs of healthcare getting bundled into patient profiles. This is really ‘phase 2 of EHRs’, and it’s roughly analogous to doctors getting bundled into health centers a century ago. And it’s pretty logical: if I’m a patient, and have various health care jobs associated with me (a broken arm last year, the flu today, an episode of anxiety next month), it makes a lot of sense for those jobs to all be linked together in one place: my personal health record, or patient profile.3
This is a necessary step, but it’s not sufficient: jobs bundled into patient profiles are a good way to organize things, but an isolated profile isn’t actually very interesting. It’s like a Facebook profile page, without the Facebook network: nice to look at, but not all that valuable. So what’s next? Some people might say ‘well the answer is a Facebook network for health!’; I don’t think it will be that straightforward. Individual patients are too unique and have too complex needs for such an idealized solution to actually work. Network business models are successful when all of its component members have the a specific set of goals; in order to get there, we need to unbundle the patient profile into those component goals first. Eat healthy; exercise more; keep my blood pressure down; manage my depression; rehabilitate my ACL; these are the goals that we all have in common with one another and can be effectively bundled into networks.
Just like last time, the first attempts to unbundle goals came at the high end; also as before, they didn’t work. Last time around, we saw the high-end specialty fee-for-outcome clinics try to unbundle specific routine and profitable procedures from the health centers. This time, it’s called a different name but is really just a digital version of the same idea: “telemedicine”. The idea that doctors could deliver routine medical care to people over the internet, in various forms – “Press a button and then my doctor appears! Just like Uber!” is appealing, but it’s clearly not happening. Like a broken record, we’re seeing the medical incumbents – physicians, clinics, providers, everyone – raise questions about patient safety and privacy (unless they’re the ones providing care, which doesn’t necessary reduce costs much) and slow down adoption significantly. Telemedicine hit the same brick wall as anyone who tries to tackle incumbents at their profit centers head on: it tried to unbundle the lucrative, high end goals (“I want personalized care at the push of a button”) instead of the low-end goals (“I want to eat healthier food”). Unbundling at the high end often seems like a great idea – Look at those amazing margins! – but usually fails in heavily-regulated environments.
So now that Phase 2 has seen our high-end unbundling attempt, what will be the Catalyst, the analog to EHRs? My guess is that it’s going to be HIPAA-compliant communication tools (Slack for healthcare, I guess). For those outside the healthcare bubble, HIPAA (the Health Insurance Portability and Accountability Act of 1996) is a set of rules that currently governs patients’ digital privacy rights. Like many government regulations, it was well thought out for its current era but whose modernizing updates have come slowly. There are a lot of people trying to improve the relationship between companies (especially startups) and HIPAA over the next few decades, and the argument that’s resonating with current health care providers is the notion that it could streamline communication between patients and their existing health care providers. This is the same playbook as when EHRs were sold to the hospitals: “it’ll help you communicate and operate more efficiently!”. And, just like with EHRs, we should hold no illusions as to whether it will be easy: it won’t. Catching healthcare up to the mobile internet will be really hard. But it’s crucial, because just like before, it is the catalyst that solves the rate limiting step for low-end unbundling.
Once these communication tools get fully integrated into the health community, my bet is that we’ll initially hear some complaining from the incumbents: most likely, something like ‘my staff had to learn all of these new apps, and it didn’t really improve my clinic at all!’ just like with EHRs in round one. But then, just like before, we’ll see health care providers quietly divest themselves of the low-end jobs that they don’t really want to be doing: getting their patients to eat healthier, exercise more, watch their blood pressure, and seek peer support groups. Those have never been moneymakers anyway, right?
When the communication barriers go away (i.e. healthcare goes full mobile internet), I’m willing to bet that the major impact won’t be visible in any kind of before/after comparison; the real benefit lies in the fact that lower-cost jobs can be unbundled off to networks with lower-cost business models. It’s the same thing we saw with the retail clinics in the previous cycle: the incumbents (who fought tooth and nail against high-end unbundling) will be happy to unbundle their time-consuming but unprofitable activities to distributed networks at the low end. We’ll have unbundled the profile, from the low end, into its component goals – which it turns out, we all pretty much have in common with one another. And then, finally, those goals will be ready to bundle into collective networks of people who all have common goals and all have common solutions. And then the magic happens: if everyone is bundled into common networks with common goals and fixed upfront costs, THAT’S WHAT SOFTWARE SOLVES. This is how software eats healthcare, how we get Airbnb and Zenefits and Uber and Facebook for healthcare. This is the playbook.
Once we reach that stage – when patient profiles get unbundled into goals and then those goals get bundled into networks – we’ll be at the point where we can sit back and let a thousand flowers bloom, software does its thing, and magical things start to happen. I don’t use the term magical lightly – I truly believe we’ll start to see health companies emerge, like Airbnb or Zenefits before them, that introduce solutions and business models that are so much better than what currently exist that it’s almost laughable. When software actually eats healthcare – none of that telemedicine or internet doctor stuff, but real low-end unbundling into networks – the results are going to be pretty great. I don’t wish to sound hyperbolic here, but I mean what I’m saying- we’re so used to health care being so dismally expensive that we can’t even understand what that kind of groundbreaking change might look like until it’s already happened. But one day, it will. And that day may be sooner than we realize.
Here are my final thoughts on “Software Eats Healthcare”:
1. Incremental improvements in health care don’t really enable disruption by software. On the other hand, bundling and unbundling – particularly at the low end – drive the powerful changes in health care that lead to real, lasting improvement.
2. The rate-limiting step right now for health care business model evolution could very well be HIPAA overhaul specifically, and patient privacy and internet accessibility generally. This isn’t going to be easy, but it may well be the most important thing we could work on for health care improvement in the grand scheme of things.
3. Just like EHRs before them, the value that these communication tools create will not actually be obvious in terms of ‘before-after’ comparisons: the value will be created at a different layer of the healthcare stack. For EHRs it meant low-end unbundling into retail clinics, for HIPAA overhaul it’ll mean low-end unbundling into health and wellness networks where software can make a big difference.
1. A brief note for health care nerds: I’m using the term ‘fee for service’ here in the American sense, to mean ‘you pay for a billing code’. I’m not using it to mean ‘as opposed to salary or capitation’, like one might encounter in the UK or some other countries with single-payer systems. Thanks for bearing with me.
2. On the payment side, we also saw payments get bundled through employers and insurers – but for this post we’re talking about what we pay for, not how we pay for it.
3. One thing I’ve noticed in common across many industries is that the bundling steps are often much easier ‘sells’ than the unbundling steps. Bundling usually makes intuitive sense: ‘all these services or payments are fragmented; let’s put them all in one place!’ Unbundling, on the other hand, tends to be less obvious and harder to predict in advance: A B and C get bundled into X, which gets unbundled into 1, 2, and 3. It requires more lateral thinking.
Join thousands of business professionals reading the Mattermark Daily newsletter. A daily digest of timely, must-read posts by investors and operators.
This is a guest post by Alex Danco, Head of Operations at Sharethebus.com. (originally posted on his blog) Have comments for this post? Tweet them to @Alex_Danco.